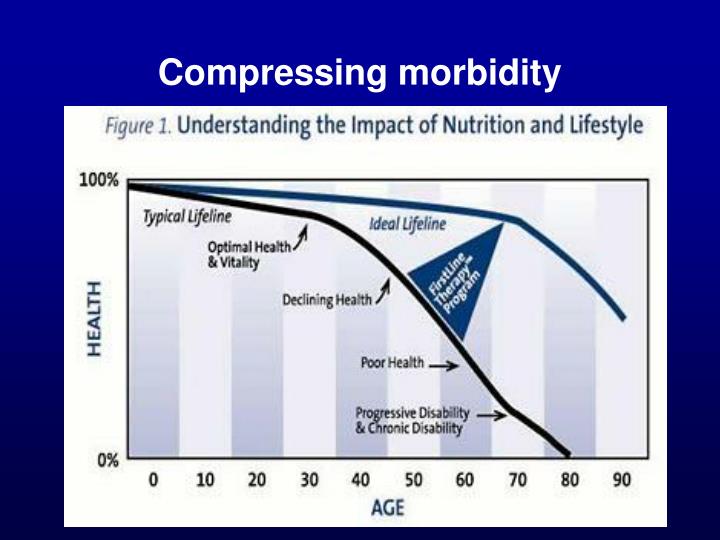
Fries’ hypothesis is that the burden of lifetime illness may be compressed into a shorter period before the time of death, if the age of onset of the first chronic infirmity can be postponed. This hypothesis contrasts to the view that as the age of countries’ populations tends to increase over time, they will become increasingly infirm and consume an ever-larger proportion of the national budget in healthcare costs.
Fries posited that if the hypothesis is confirmed, healthcare costs and patient health overall will be improved. In order to confirm this hypothesis, the evidence must show that it is possible to delay the onset of infirmity, and that corresponding increases in longevity will at least be modest. The evidence is at best mixed. Vincent Mor’s “The Compression of Morbidity Hypothesis: A Review of Research and Prospects for the Future” argues that “Cross-national evidence for the validity of the compression of morbidity hypothesis originally proposed by Fries is generally accepted. Generational improvements in education and the increased availability of adaptive technologies and even medical treatments that enhance quality of life have facilitated continued independence of older persons in the industrialized world. Whether this trend continues may depend upon the effect of the obesity epidemic on the next generation of older people. See also “Mortality and Morbidity Trends: Is There Compression of Morbidity?” for recent evidence against the hypothesis.”
Just find this interesting and a great reason to maintain or stay at a healthy (weight) for a longer length of time.
Higher Intake of Omega-3s Lowers Diabetics’ Mortality Risk
People with diabetes who had a higher intake of the omega-3 fatty acids, EPA and DHA had a lower risk of all-cause mortality compared to diabetics whose intake was lower, a study in Acta Diabetologica reported.
The clinical study included 4,854 diabetic participants in the National Health and Nutrition Examination Survey 1999-2014. Mortality data were obtained through 2015.
During the follow-up, 1102 deaths occurred. People whose intake of EPA and DHA was among the highest 20% of participants, at more than 122 mg per day, had a 25% lower risk of mortality from any cause compared to those whose intake of the fatty aids was among the lowest 20%, at 9.5 mg or less.
When the risks of all-cause mortality associated with EPA and DHA were analyzed separately, greater DHA intake emerged as significantly associated with lower mortality risk. As in all nutrition studies, more research is needed.
EPA = eicosapentaenoic acid (a long-chain fatty acid Omega-3) DHA = decosahexaenoic acid (a long-chain Omega 3)
Although life span has not changed, life expectancy has increased dramatically over the past century.
With rare exceptions, life expectancy has been on the rise in the U.S. It was 47 years in 1900, 68 years in 195v0, and by 2019i it had risen to nearly 79 years. But it fell to 77 in 2020 and dropped further to just over 76 in 2021. (can you think Covid?) Harvard Health.
The causes of aging are still a mystery.Most likely, aging results from an interaction of genetic and the changes listed in the table below: The science of epigenetics also can offer lifestyle factors to further influence the changes that normally occur with “normal aging”.
Aging occurs due when: Errors occur in copying the genetic blueprint (DNA) Connective tissue stiffens. Parallel muscle proteins cross link. Electron – seeking compounds (free radicals) damage cell. Hormone functions change. Blood glucose attaches to various blood and body proteins. Occurs in poorly controlled diabetes The immune system loses some efficiency and fails to recognize foreign substances. Autoimmunity develops. Immune function cells destroy “self”. Death is programmed into the cell, e.g. each cell can only divide about 50 times; after that the cell dies and succumbs. Excess energy intake speeds body breakdown and may even cause premature death. In research, underfed animals live longer by calorie restriction. Diet can slow down some of these processes? Source: Gordon M. Wardlaw. Contemporary Nutrition: Issues and Insights. Page 518-520. Edited for Food, Facts and Fads by: Sally J. Feltner, MS, PhD
WOW!!! What else could go wrong?
Healthy lifestyles may be found to alleviate some or all of these body processes.
How to Reverse Prediabetes. It is surprisingly easy to stop this condition from developing into full-blown diabetes. By Jill Weisenberger, M.S, RDN , CDCES Nutrition Solutions Bottom Line Health Adapted from Food, Facts and Fads
More than 96 million American adults have prediabetes — Blood sugar levels lower than type 2 diabetes but higher than normal. However, there is good news. Decades of research tells us that reversing prediabetes by restoring your blood sugar to normal levels if possible by making a few lifestyle adjustments. Much comes the results of a program called the Diabetes Prevention Program (DPP), a – 3 year-long study with 3,000 ,participants. Prediabetes has no obvious symptoms, only a few metabolic markers that can tell us how progressive the disease may be in time. It’s more likely if you have excess weight, smoke, are inactive, sleep poorly, have high blood pressure, low (good) HDL cholesterol, or heart disease. These factors become suggestive that these risk factors should be tested and monitored for susceptibility to diabetes type 2. If you discover that you have prediabetes (preferably there are some things you can do: improve your diet, increase your activity, and lose a little weight (if overweight) all with the permission of your primary care physician and assessment of the above risk factors.Improve Your Diet There is no best diet to lower high blood sugar. Rather, you should eat nutrient-dense foods like fruit, vegetables, whole grains, beans, nuts, lean meats, fish, and low fat and non-fat dairy (no surprises there!!!) However, there is one category you should avoid: sugar sweetened soft drinks, fruit drinks, energy drinks, sports drinks, sweetened teas, and coffee beverages with added sugar. Watch the snacks – our diets are often snack heavy which encourages the intake of highly processed foods loaded with carbs, salt, fat and sugar. Stay away from keto, low fat, low carb, low fat- all these “diets” require willpower or deprivation of some kind that encourages binge eating. Increase activity
Keep it simple – avoid gyms and exercise programs (unless you are highly structured and motivated. “Enjoy walking? If you do, set aside at least 5 minutes every day rather than longer periods just two or three times weekly. A daily behavior is more likely to become a habit. Gradually increase the daily time you spend walking, until you’re walking about 20 to 30 minutes every day.”
Lose a Little weight“
In one study, people at high risk for developing type 2 diabetes who lost just 5 percent of their body weight improved the function of their pancreatic beta cells and decreased insulin resistance. Use small dishes (9 inches) Eat from a dish – no reaching into boxes or bags” Sometimes just a few small changes can make a big difference.
In a study on longevity in women, researchers from the University of California San Diego (UCSD) examined the benefits of keeping a stable weight for older women.
The scientists studied data from thousands of women to determine the likelihood of reaching the ages of 90, 95, or 100, which they called “exceptional longevity.”
Their data analysis showed that older women who maintained a stable weight may be 1.2 to 2 times more likely to reach ages 90 to 100.
While maintaining a stable weight provided benefits toward reaching exceptional longevity, unintentional weight loss was associated with a decrease in the likelihood of reaching 90.
Older women looking to extend their lifespan to the age of 90 or beyond should focus on maintaining a stable weight.
A recent multi-institutional study found that older women who maintained a stable body weight after 60 were more likely to reach their 90th birthdays.
The study involved 54,437 women from the Women’s Health Initiative. The researchers looked at short-term and long-term weight changes in women and compared that to the age they reached.
The researchers found that women who experienced unintentional weight loss had 51% lower odds of reaching 90.
While weight loss was associated with decreased longevity, a weight gain of 5% or more did not contribute to exceptional longevity, which points toward the importance of maintaining a stable weight.
This study aimed to analyze any associations between weight changes (intentional or unintentional) and exceptional longevity in older women.
The authors noted that prior studies analyzed the effects of weight loss in early to middle adulthood, such as shifting from being a person with obesity to being overweight, but that these studies had not considered whether the weight loss was intentional.
The UCSD study included nearly 55,000 postmenopausal women who participated in the Women’s Health Initiative (WHI) study, which began in 1991. The WHI study focused on health issues in postmenopausal women, such as heart disease and cancer.
The authors chose to use data from women who were ages 61 to 81 at the time of enrolling in the study. The women provided information, including their weight, medical conditions, alcohol consumption, and smoking status.
The researchers looked at weight changes from the beginning of each participant’s enrollment and later at the 3-year and 10-year marks. They categorized the women into one of three groups:
Stable weight (less than 5% change from starting weight)
Weight loss (more than 5% decrease from starting weight)
Weight gain (more than 5% increase from starting weight)
The authors also classified the women into “intentional weight loss” or “unintentional weight loss groups” at the 3-year weigh-in, depending on whether they reported losing more than 5 pounds on purpose.
After excluding any women who died within the first year of the 3-year weigh-in (to avoid pre-existing health conditions impacting results), the researchers found that 56.3% of women who maintained a stable weight lived to be at least 90 years old.
Women who experienced unintentional weight loss of 5% or more were less likely to reach the age of 90.
According to the authors, women who had weight loss (for any reason) of more than 5% at the 3-year checkup had 33% lower odds of reaching 90, 35% lower odds of reaching 95, and 38% lower odds of reaching 100.
They also looked at whether the weight loss was intentional or unintentional, and the women who tried to lose weight had 17% reduced odds of reaching 90. Some reasons for intentionally losing weight included diet changes and an increase in exercise.
The women who did not lose weight on purpose had 51% reduced odds of reaching 90. Some reasons the women reported for unintentionally losing weight include illness and stress.
Alternatively, a weight gain of more than 5% at the 3-year weigh-in was not associated with increased chances of survival.
“It is very common for older women in the United States to experience [being overweight or having obesity] with a body mass index range of 25 to 35. Our findings support stable weight as a goal for longevity in older women,” says Professor Aladdin H. Shadyab, the study’s lead author and professor at UCSD’s School of Public Health and Human Longevity Science.
The Most Successful Diets (Based on Nutrition Experts).
For the last 13 years U.S. News and World Report has selected a panel of health and nutriiton experts to determine which works well for individuals with diabetes, those interested in weight loss, and people with a family history or other risk factor for heart disease and more.
After examining 24 diets, the ones that scored the highest and were selected as eating plans that more people might find success with checked most of these boxes: Tasty Flexible Convenient Filling Feature nutrient-rich foods and all food groups Adaptable to the whole family or household
Diets that fell near the bottom checked the following: Require rigid eating schedules or menus Call for bland food Tend to emphsize unfamilar ingredients or specialty products Involve challenging restrictions Elminate entire food groups or severely restrict calories.
The Top Five: Flexitarian Diet Mediterranean Diet Mayo Clinic Volumetrics MIND
The Bottom Five Optavia Raw Food Keto (sorry-very restrictive) Jenny Craig
Slim Fast
The Bottom Line The diets that were rated as easist to follow offered a lot of variety, were convenient and encouraged foods that reduce risk for disease, support balanced energy levels and are simply fun to eat.
The best diet strategy of all is one that adds to your quality of life, rather than subtracts from it.
Source: By Karla Walsh – Published: January 6, 2023 Reviewed by Jessica Ball, M.S. RD Eating Well Magazine The Blue Zones Solution; Eating and Living Like the World’s Healthiest People. Dan Buettner
Higher Intake of Omega-3s Lowers Diabetics’ Mortality Risk
People with diabetes who had a higher intake of the omega-3 fatty acids, EPA and DHA had a lower risk of all-cause mortality compared to diabetics whose intake was lower, a study in Acta Diabetologica reported.
The clinical study included 4,854 diabetic participants in the National Health and Nutrition Examination Survey 1999-2014. Mortality data were obtained through 2015.
During the follow-up, 1102 deaths occurred. People whose intake of EPA and DHA was among the highest 20% of participants, at more than 122 mg per day, had a 25% lower risk of mortality from any cause compared to those whose intake of the fatty aids was among the lowest 20%, at 9.5 mg or less.
When the risks of all-cause mortality associated with EPA and DHA were analyzed separately, greater DHA intake emerged as significantly associated with lower mortality risk.
EPA = eicosapentaenoic acid (a long-chain fatty acid ) DHA = decosahexaenoic acid (a long-chain fatty acid)
Every once in a while, it is fun to go back into history and rediscover the fads that were popular then – the story of Bernaar MacFadden is one of them. He was however, very successful and in my opinion, a very fascinating human being.
“In 1913, twenty year old Mary Williamson, a runner and muscular swimmer was crowned “Great Britain’s Perfect Woman and as part of her prize was a job offer from fitness guru, forty-four year old, Bernarr MacFadden. The job involved a traveling physical fitness show billed as “The World’s Healthiest Man and Woman.” They performed feats of physical prowess with the big finale featuring Mary’s nightly jump from a seven-foot platform onto MacFadden’s stomach. Another “prize” was becoming Bernarr’s third wife. He proposed one day when the pair was halfway through a ten-mile run and when she accepted, she recalled: “He stood on his head on me for one minute and four seconds.” Who was this man?
EARLY YEARS
Bernarr MacFadden was a man that brought physical culture to America and Europe. “He stood five foot six inches tall and built a fortune from often, but not totally, misinforming the public about nutrition and health.. He was born in 1868 on a farm near Mill Springs, Missouri where his father died when he was four from chronic alcohol consumption.
Bernarr, a sickly boy, was raised by a TB-ill mother who sent him away to a cheap boarding school. He later referred to this school as the “starvation school”. Bernarr remembered often having peanuts as his only source of nourishment. His mother died from tuberculosis when he was eleven and Bernard, (he changed his name later to Bernaar) was sent to a northern Illinois farm to work for two years where his heath improved. He was then shipped off to St. Louis where his waiting relatives welcomed him, namely Uncle Harvey.
When walking in downtown St. Louis with his uncle one day, he discovered the Missouri Gymnasium and was impressed by the posters of musclemen displayed there. “The sickly young Barnard swore an oath: I’m going to be like them. I’m going to look like them.”
Bernarr obtained a copy of How to Get Strong and Stay So, a bestseller in 1879 written by William Blaikie, a strongman and endurance athlete. He was further inspired to follow his dream; therefore, in the spring of 1891, Bernarr hung a shingle out that read:
“BERNARR MCFADDEN – KINISITHERAPIST
TEACHER OF HIGHER PHYSICAL CULTURE”
He declared himself a “teacher of physical culture” to become the nation’s first personal trainer. He made up the term, kinisitherapist. No one knew what he meant.
BELIEFS
MacFadden’s core belief mimicked the philosophy of Sylvester Graham that blamed toxins, improper diet and exercise habits, lack of sunshine and the use of tobacco and alcohol to be the reasons for most diseases. Bernard despised white flour and called it “dead food” and said: “ I saw that white bread was frequently condemned and I whenever available, secured whole wheat or Graham bread.” He did not, however, carry on the sexual restrictions of Graham.
He began a lecture series on physical culture and put up posters and small ads in the local newspapers. Each lecture started with Macfadden dressed only in a loincloth posing artistically in front of a cabinet lined with black velvet and lit from below to make him appear larger than he was. His lectures became popular in both the U.S. and Europe.
He taught his nation-wide audiences that fresh fruits, vegetables, and whole grains were vital to good health. Today we know that his teachings about diet were relatively accurate in an era when nutrition knowledge was meager. He was not a true vegan, but used meat sparingly. His favorite food was carrots and he dutifully avoided sugar foods such as candy, cakes, pies and ice cream. He advocated eating only two meals a day and preached moderation while fasting once a week. There are some advocates that now suggest the same regimen. He did not believe in pasteurization or homogenization of milk. He said that milk could cure many diseases. He avoided alcohol, tobacco. Of course, he advocated brisk walking, lifting weights, and prescribed calisthenics. Today’s body builders consider him the “father of physical culture.”
MacFadden published a culture magazine called Physical Culture. In 1901, he wrote: “Every disease in the human body is simply an endeavor on the part of the body to correct an abnormal condition…. It is the presence of impurities in the blood that make the production of a cold possible…Disease germs consume these poisons, or render them harmless.” By 1910, he ruled over a physical fitness empire. The empire included spas called “healthatoriums”, Physical Culture City and then Physical Culture University. He continued by promoting raw foods and salads every day and used fresh fruits to keep the intestines “antiseptic” to avoid autointoxication. He continued to avoid processed white sugar and flour.
LATER YEARS
His empire began to crumble. Research led to more knowledge about food components such as vitamins and minerals in the nutrition field. People began to lose interest in MacFadden’s ideas and his popularity declined.
In the final decade of his life, his previous wealth dwindled. He did not give up, however. He jumped out of a plane on his 83rd birthday; he did the same stunt the next year. In 1955, he was 87 and was experiencing liver and urinary tract problems. He fasted to treat his condition, but ironically died three days later due to complications from jaundice and dehydration.
LEGACY
Bernaar MacFadden was one of the most flamboyant and bizarre personalities in American culture; yet many people have forgotten him or have never heard of him today. He was the first food crusader to be known internationally and single-handed created the health and fitness awareness for millions of people. He continued to support detoxing and fasting that carried on the principles of Sylvester Graham. Even though some considered him a “quack,” he fought against medical quackery that began in the early 20th century. At the same time, he supported the medical practices of chiropractic and osteopathic treatments. In many aspects of his career like publishing and advertising, he was truly a genius.
In England, William Banting consulted Dr. William Harvey for weight loss who recommended he cut most sugar and starch from his diet since foods containing those substances tend to create body fat. He lost 50 pounds and wrote the first diet book, “Letter on Corpulence Addressed to the Public” in 1862.
1898
Horace Fletcher loses 42 pounds by advocating that we need to chew food about 32 to 80 times before being swallowed and it should be in liquid form. He later became known as “The Great Masticator”.
1918
Dr. Lulu Hunt writes the first best selling diet book, “Diet and Health with a Key to the Calorie”. She promoted calorie counting over her entire life.
1919
The Continental Scale Company produces the first bathroom scale called the “Health O Meter”.
1929
A cigarette advertisement tells women to “reach for a Lucky instead of a sweet”. Another slogan says: “Light a Lucky and you’ll never miss sweets that make you fat”.
1930
The “grapefruit diet” also known as “The Hollywood Diet” is promoted which involves eating only 585 calories a day for 18 days with boiled eggs, green vegetables and Melba toast.
1936
Self-proclaimed diet guru Victor Lindlahr reaches thousands via the radio to produce his regular broadcasts entitled “reducing party”. He wrote the book You Are What You Eat, one of the earliest texts of the health food movement in the United States, which sold over half a million copies and introduced the phrase still used today.
1942
The Metropolitan Life Insurance Company published standard weight tables for “ideal weight”. The charts used weight, height, frame size, and gender but only used data from life insurance policyholders.
1948
Amphetamines were first prescribed for some obese patients but later research determined that these were dangerous. Amphetamine –like drugs are still used today in a limited fashion.
1958
Saccharin, the first manufactured artificial sweetener is produced and becomes a popular sugar substitute. It is still used today after years of research that absolved critical reports of its cancer connection.
1961
Weight Watchers was born as a result of Jean Nidetch and several friends who met in her apartment to offer each other support about dieting.
1967
Twiggy, 5’7” and weighing about 92 pounds becomes a supermodel and icon for the slender female.
1972
Dr. Atkins introduced his first “Diet Revolution”, a high protein, high fat, low carbohydrate diet.
Richard Simmons opens Ruffage and the Anatomy Asylum, a Beverly Hills restaurant and exercise studio. He quickly becomes known as a fitness and diet guru.
1978
Dr. Herman Tarnover introduces the “Complete Scarsdale Medical Diet”, another version of the high protein, low-carb diet.
1979
The Pritikin Diet answers the trend of the high protein, low – carb diets with a high fiber, very low fat diet. The system was originally designed for heart patients but became popular for those who followed the newer trend of the low –fat diet approach.
1981
The Beverly Hills Diet is introduced – it recommends eating nothing but fruit for the first 10 days.
1982
Aspartame is introduced as another alternative sugar substitute. It was marketed as NutraSweet and is still used today in many products.
Liposuction is performed in the U.S. for the first time and now becomes a popular cosmetic procedure for the obese.
1983
Jenny Craig is formed which sells their own line of diet foods and offers diet counseling. Nutrisystem soon followed.
1988
Oprah Winfrey loses 67 pounds on the liquid diet Optifast.
1994
The FDA mandates that food labels must include detailed information about calories, fat, and fiber. We must thank Dr. Lulu Hunt Peters for this.
1995
“The Zone Diet” is introduced by Dr. Barry Sears. He promotes eating lots of fruits and vegetables and protein, while cutting back on breads and pastas.
1996
It is reported that 40% of nine and ten-year-olds are dieting and trying to lose weight.
2000
Experts are stating that there is now a global epidemic of obesity and that for the first time in history, this number of overweight people equals the number of underfed and undernourished.
2002
Dr. Atkins introduces his second diet book, the “New Diet Revolution” to a new generation of dieters. The Low-carb diet is back after multitudes of diet books promoting low fat diets.
2013
It appears we may have come full circle – we are now promoting cutting sugars and counting calories (again). We have progressed from low carbohydrate, low fat, and low carbohydrate diets again along with some pretty scary schemes, e.g. the tapeworm diet. Many weight loss books, gimmicks and pills have come and gone over and over again and many still exist, but with no real breakthroughs. I doubt they will not end at least in the near future – what do you think?
2023
For the last 10 years, we as a culture have waged a new diet war – Keto diet, paleo diets are the latest “experiments,” trending to the low carb side with higher fat – right back where we started. According to Bittman and Katz, “everything we learned in the late 20th century, the range for fat is considerably broader.” There are claims for good outcomes with diets that have 10% or less of calories from fat (like in Okinawa); those would be the low fat-diets. There are the Mediterranean diets that get well over 40% of their calories from fat and seem to produce the same great health outcomes.” (Mark Bittman and David L. Katz, M.D. How to Eat: All Your Food and Diet Questions Answered.)
Source:
James Trager(1995) The Food Chronology: A Food Lover’s Compendium of Events and Anecdotes, From Prehistory to the Present.
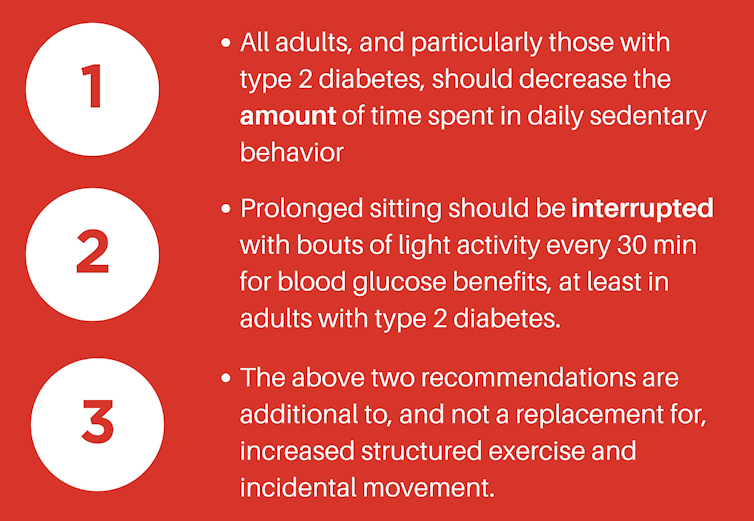
Adults are sitting more than ever, and few pay attention to how they sit throughout the day.
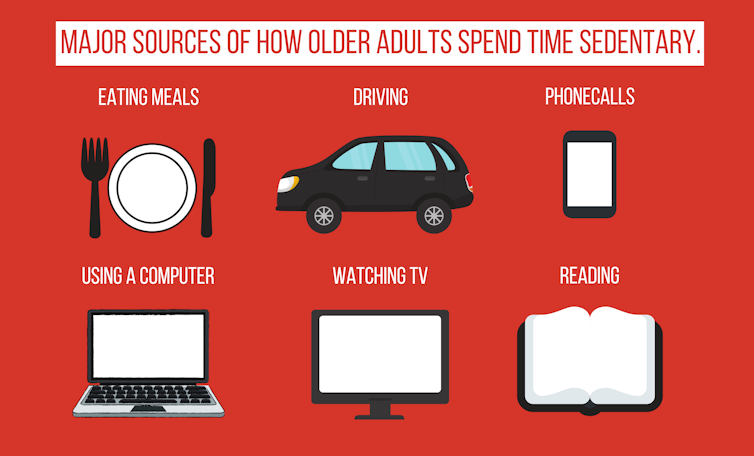
Take a moment to think about all the reasons we sit. First off, you’re probably sitting while reading this. Some of the most common sitting activities include eating meals; driving; talking on the phone; using a computer, television, or small device; and reading. Now take another moment to think about all the sitting done across your lifetime.
The fact is, the amount of time spent sitting has increased over time. And with innovations such as Alexa, delivered groceries, and pre-made meal services, we expect many older adults will sit longer and will do it more often. As of today, the averageolderadultspendsbetween56 percent and 86 percent of their waking day sedentary. That’s a lot of sitting.
Our research team studies healthy aging and is interested in how sitting too much might contribute to heart disease and diabetes. Our recent study suggests that the way older adults accumulate their sitting time might be important for aging without diabetes.
“…the way older adults accumulate their sitting time might be important for aging without diabetes.”
What happens while sitting?
When you sit for long periods without getting up, the large weight-bearing muscles of the legs remain dormant. With no action, these muscles are unable to efficiently use the sugars and fats that float around in your blood – and in theory, this could lead to weight gain and metabolic diseases such as diabetes.
At the same time, reduced blood flow in your arteries leads to hostile conditions that promote injury to the blood vessel walls. Over a lifetime, this injury likely contributes to heart disease and to peripheral artery disease. Furthermore, when your leg muscles remain shut off for long periods, blood collects in your veins which leads to an increased risk for blood clots, or deep venous thrombosis. Standing up and moving around can stop these processes, but all too often, we just keep sitting.
Blood flow can become ‘turbulent,’ causing damage to arteries. www.pexels.com
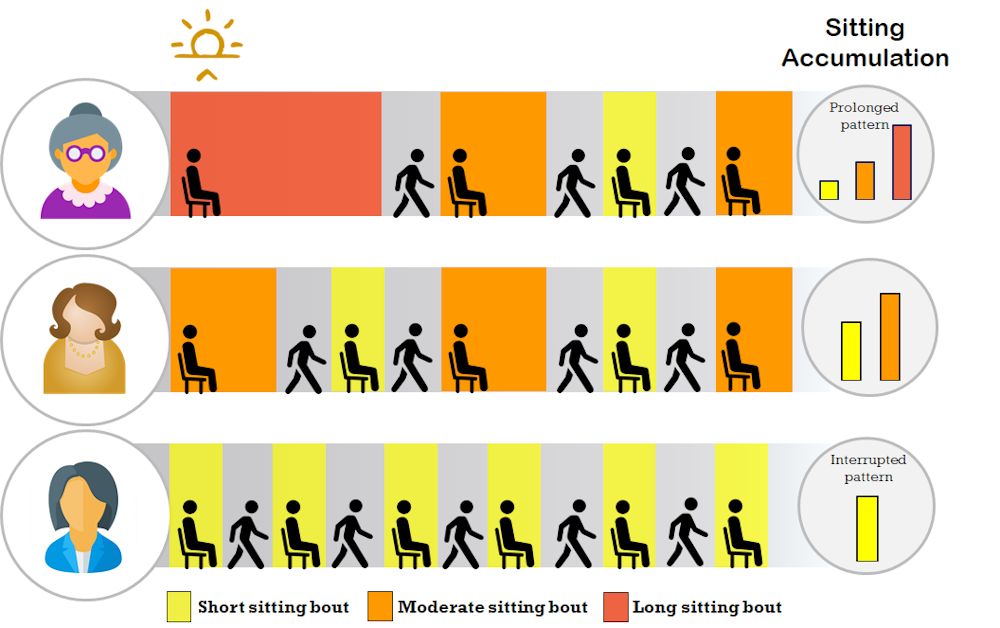
Sitting patterns
Sitting patterns describe how people sit throughout the day. Some people commonly sit for long periods at a time, rarely getting up. They are said to have prolonged sitting patterns. Others rarely sit still. They regularly get up after sitting for just short periods. These sitters are said to have interrupted sitting patterns. Where do you fit on the sitting pattern spectrum?
To test whether problems with fat and sugar metabolism were being caused by sitting patterns, researchers around the world conducted experiments. They brought adults into a laboratory at least two times each, having them sit continuously for about eight hours (an extremely prolonged pattern). On the second day, the participants were asked to get up every 20-30 minutes (a highly interrupted pattern). The interruptions lasted for two to five minutes and included standing still, light walking, simple resistance exercises or moderate-intensity walking, depending on the study.
When researchers synthesized evidence from most of the laboratory studies, the results were clear. On days with prolonged patterns, our bodiesarenot able to metabolize fats or sugar as well as they are on days with interrupted patterns. Blood pressure and fatigue were also higher on days with prolonged sitting compared to days with interrupted patterns.
These groundbreaking laboratory studies provided strong evidence that sitting patterns had an immediate effect on how the body processes fats and sugar, otherwise known as metabolism. This led to the idea that prolonged sitting patterns over a lifetime could contribute to metabolic diseases such as diabetes in later life. Since diabetes can take a long time to develop, this question cannot be feasibly tested in a laboratory. Instead, we turned to an observational study of the population to help answer the question.
Are sitting patterns related to diabetes?
We recruited over 6,000 women aged 65-99 from the Women’s Health Initiative and measured their sedentary patterns for seven days using research-grade activity monitors. We also had over 20 years of detailed health records, which included information on whether the women had ever been diagnosed by a physician with diabetes.
As expected, the group with the most prolonged sedentary patterns had the most women with diabetes. The group with the most interrupted patterns had the fewest women with diabetes.
We used advanced statistical procedures to account for differences in other factors such as dietary habits, physical activity, medication use, weight, age, alcohol and cigarette use, and overall health, giving us more confidence that the sitting patterns were, in fact, driving the findings. We should caution, however, that since we did not measure sitting patterns before the women were first diagnosed with diabetes, we do not know whether the sitting patterns contributed to diabetes or whether the diabetes changed their sitting patterns. We ran additional statistical tests to try to untangle that, which indicated that sitting patterns contributed to diabetes. However, additional studies specifically suited to answer the question of causation are needed.
Based on the findings from our study and those of the Dutch researchers, when viewed with the earlier epidemiologic data and findings from the laboratory experiments, it seems that sitting patterns may contribute to the growing international diabetes epidemic.
With that said, as with all science, these first few studies are only the beginning of the story. Much more work lies ahead. For the time being, there is a possibility that changing your sitting patterns might provide protection against diabetes, especially if long sitting bouts were always broken with light activity or even better, moderate-intensity activity, as recommended by the American Diabetes Association.
The authors wish to sincerely thank Dr. Jonathan Unkart for his help with this story.
John Bellettiere is a postdoctoral scholar at the University of California San Diego studying Family Medicine and Public Health. Andrea LaCroix, PhD, is Professor and Chief of Epidemiology, Family Medicine and Public Health at the University of California San Diego. She received her PhD in Epidemiology from the University of North Carolina at Chapel Hill and completed a postdoctoral fellowship in cardiovascular disease at The Johns Hopkins University. Matthew Mclaughlin is a PhD student at the University of Newcastle in Australia and a research assistant at Hunter New England Population Health.